
Picking Bottle Nipples for the Breastfed Baby
With Amy Peterson, IBCLC This post made possible by the support of EvenFlo Feeding ________________________ Lots of breastfed babies will also use a bottle. Most of us have heard that introducing…

With Amy Peterson, IBCLC This post made possible by the support of EvenFlo Feeding ________________________ Lots of breastfed babies will also use a bottle. Most of us have heard that introducing…

There’s a simple way to prevent and ease some pumping discomfort, long time Leaky and WIC Breastfeeding Peer Counselor Kristine Phillips Keller shares what she has learned to help other moms that are pumping their breastmilk. This practical tip was a game changer In Kristine’s own journey as an exclusively pumping mom for her little guy.
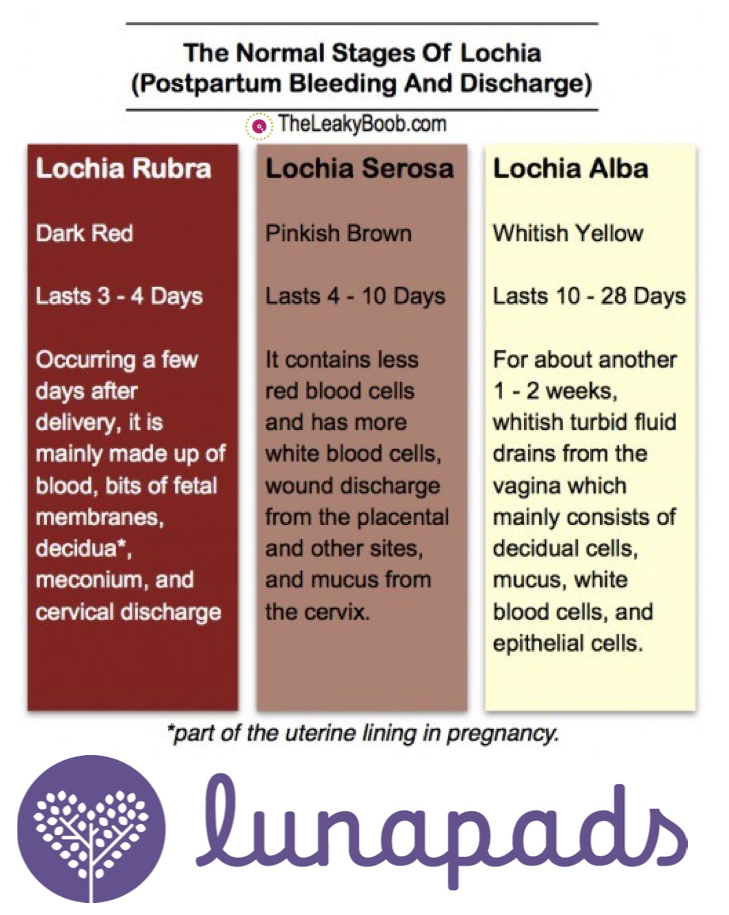
by Dr. Kymberlee Lake Most women know that there may be some bleeding after giving birth but often women are surprised by how much and how long and they…

By Amy Peterson, IBCLC This article made possible by the generous support of Earth Mama Angel Baby. Not every mom needs to pump. When baby is with mom for feedings…

by Shari Criso, RN, CNM, IBCLC This post made possible by the support of EvenFlo Feeding ____________________ Can I breastfeed throughout my pregnancy? Breastfeeding during pregnancy is very normal. Throughout…

by Shari Criso, RN, CNM, IBCLC This post made possible by the support of EvenFlo Feeding [youtube https://www.youtube.com/watch?v=mFYB_paJVmw&w=600&h=338 ] When it comes to breastfeeding, one of the myths that drives…
