
Having Enough Milk for Your First Day Back
by Shari Criso, RN, CNM, IBCLC This post made possible by the support of Evenflo Feeding ____________________ [vimeo https://vimeo.com/153279519 w=600&h=338] As you are preparing to return to work, you’ll…

by Shari Criso, RN, CNM, IBCLC This post made possible by the support of Evenflo Feeding ____________________ [vimeo https://vimeo.com/153279519 w=600&h=338] As you are preparing to return to work, you’ll…
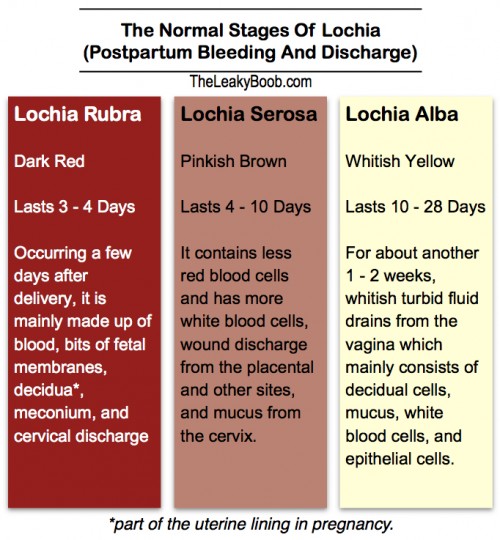
by Dr. Kymberlee Lake Most women know that there may be some bleeding after giving birth but often women are surprised by how much and how long and they aren’t…

by Tanya Lieberman This post was made possible by the generous support of MotherLove Herbal Company. Having intrusive thoughts about your birth? Flashbacks? Feeling disconnected from your baby? Do you steer…
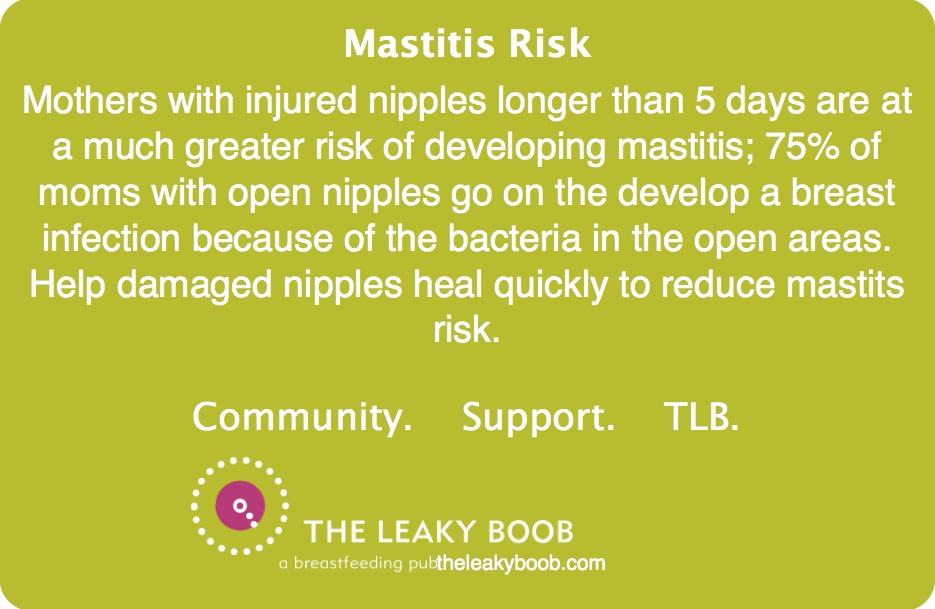
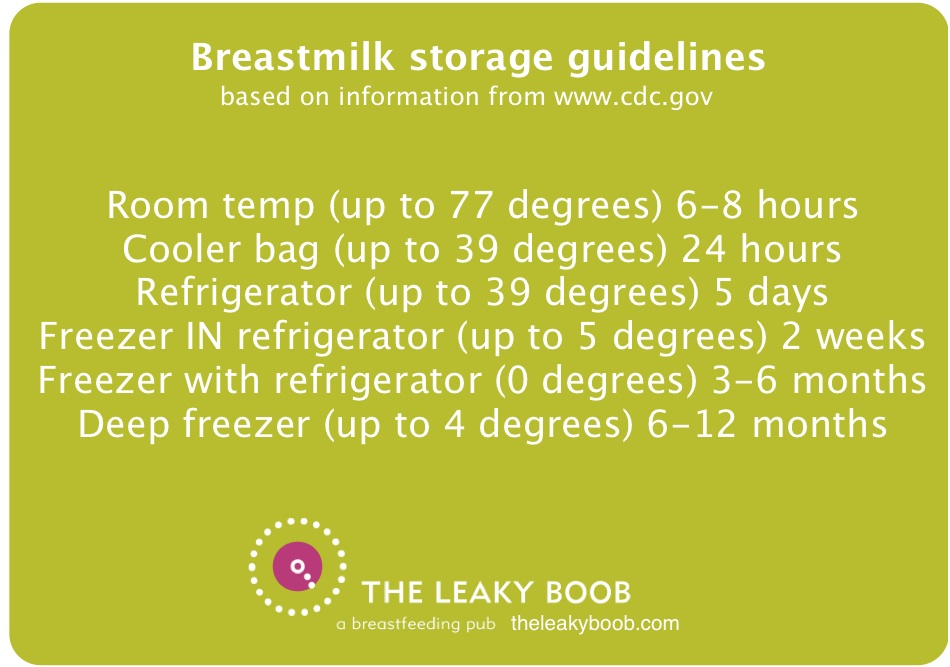
IBCLC and author Kathleen Huggins answers questions about thrush, nipple damage, and pumping to maintain supply while healing.

Daily, we receive hundreds of emails and messages from Leakies looking for help and information in their breastfeeding journey. As so many seek support from us, we are so honored…
TLB friend and supporter, Kathleen Huggins, IBCLC and author of The Nursing Mothers’ Companion, answers questions about breastfeeding, bottle feeding, pumping, and relacating.
